Printable Ub04 Form
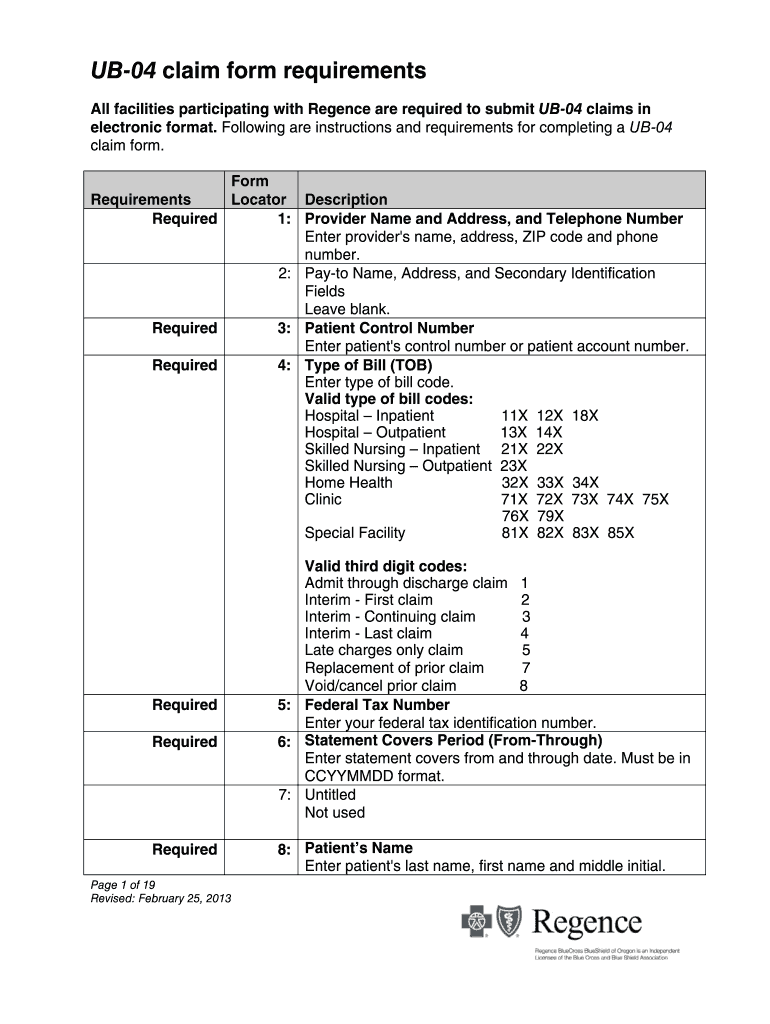
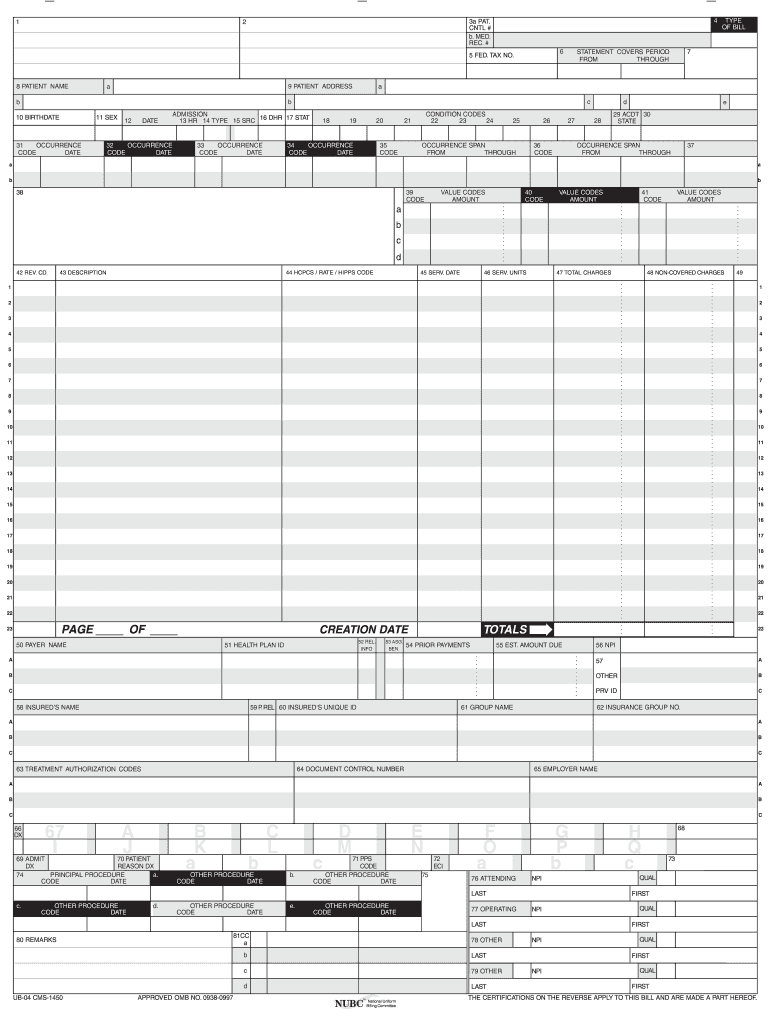
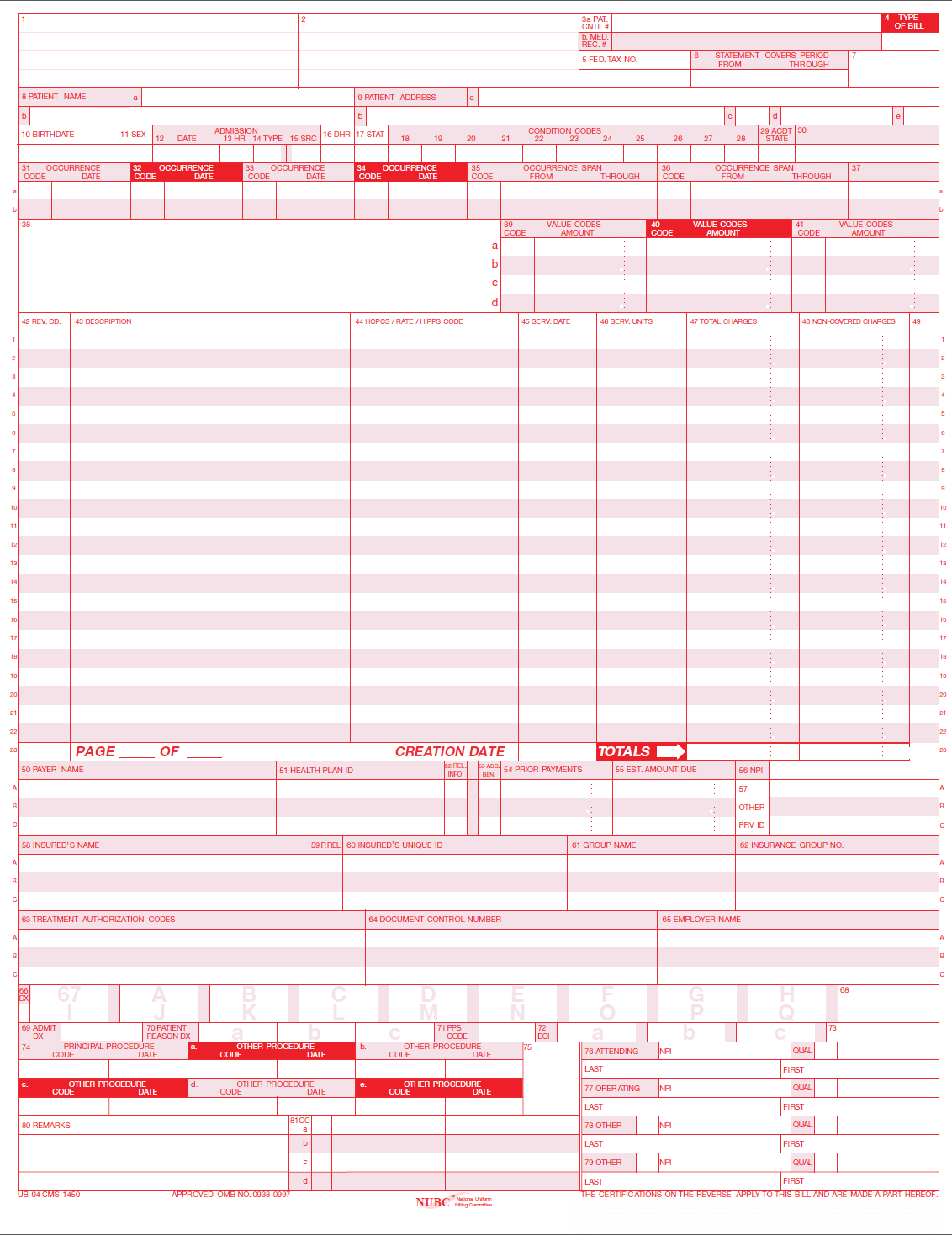
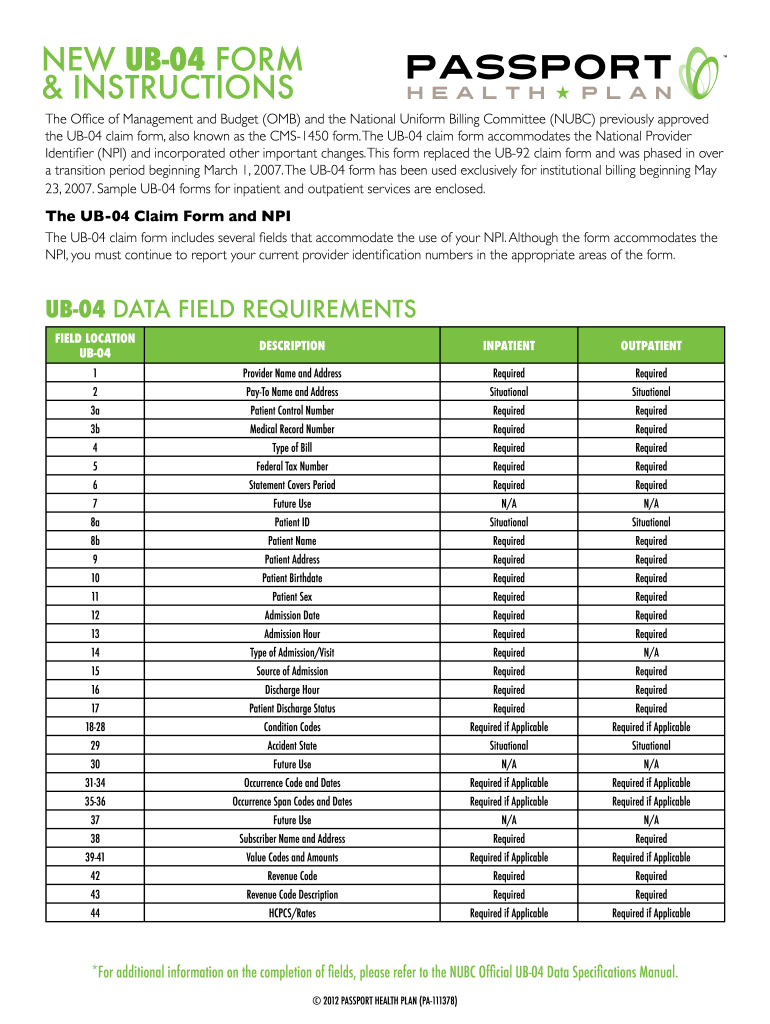
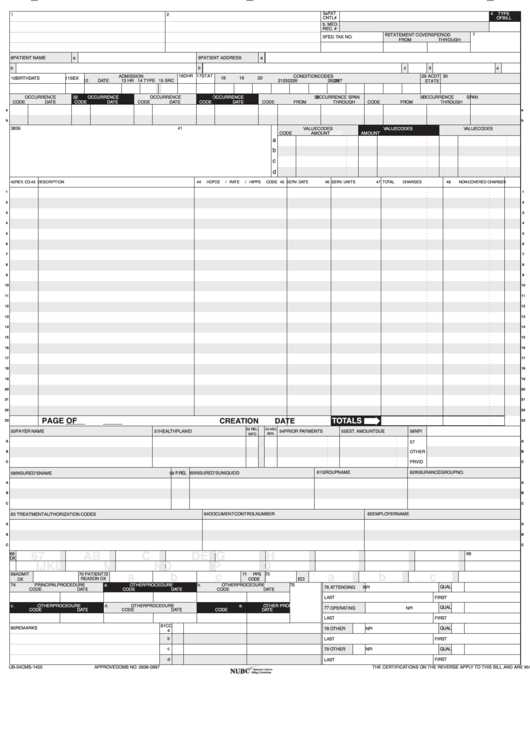
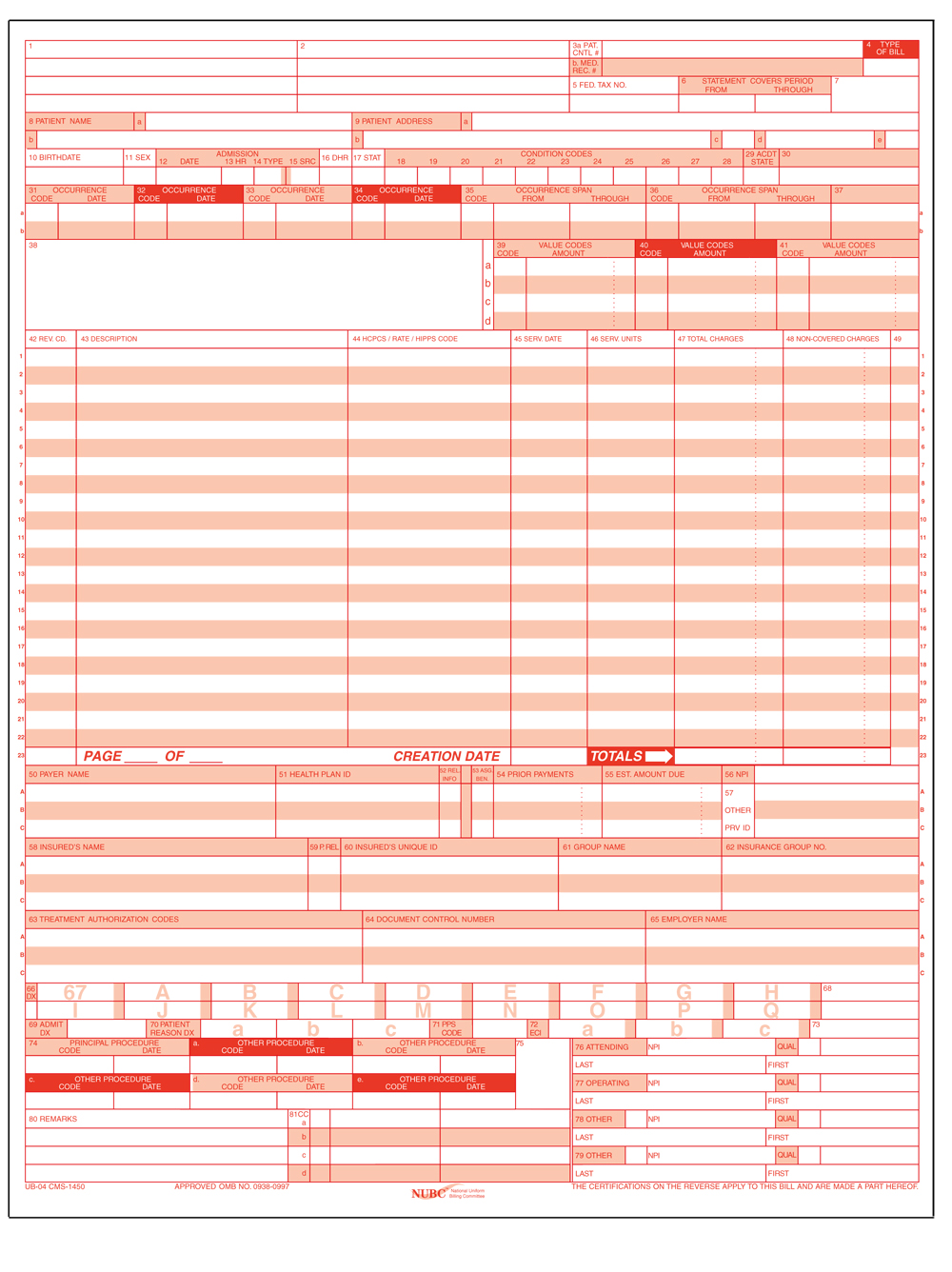
Printable Ub04 Form - We are providing two different versions in. You can fill in the attached forms electronically, using adobe form filler, as long as you have adobe acrobat reader. • inpatient hospital facilities, such as medical/surgical intensive. This number will be printed on the ra and will help. Online customers supportpaperless workflowfree trialcancel anytime Web of essential information as requested by this form, may serve as the basis for civil monetarty penalties and assessments and may upon conviction include fines and/or. Billing provider name & address. Enter the billing provider’s name, street address, city, state, and zip code where the services were performed. Enter the name and address of the hospital/facility submitting the claim. Web learn how to fill out the ub04 form for health insurance claims with this online tutorial from mcgraw hill education. We are providing two different versions in. Online customers supportpaperless workflowfree trialcancel anytime Web the ub04 claim form is used to submit claims for inpatient and outpatient services by institutional facilities (for example, outpatient departments, rural health clinics, chronic. Enter the billing provider’s name, street address, city, state, and zip code where the services were performed. Enter the billing provider’s. Online customers supportpaperless workflowfree trialcancel anytime Billing provider name & address. Web patient control number enter your facility's unique account number assigned to the patient, up to 20 alpha/numeric characters. • inpatient hospital facilities, such as medical/surgical intensive. You can fill in the attached forms electronically, using adobe form filler, as long as you have adobe acrobat reader. Online customers supportpaperless workflowfree trialcancel anytime We are providing two different versions in. This number will be printed on the ra and will help. You can fill in the attached forms electronically, using adobe form filler, as long as you have adobe acrobat reader. Enter the billing provider’s mailing. Billing provider name & address. Enter the billing provider’s mailing. • inpatient hospital facilities, such as medical/surgical intensive. Enter the billing provider’s name, street address, city, state, and zip code where the services were performed. Enter the name and address of the hospital/facility submitting the claim. Online customers supportpaperless workflowfree trialcancel anytime Web patient control number enter your facility's unique account number assigned to the patient, up to 20 alpha/numeric characters. Web of essential information as requested by this form, may serve as the basis for civil monetarty penalties and assessments and may upon conviction include fines and/or. You can fill in the attached forms electronically,. We are providing two different versions in. Web the ub04 claim form is used to submit claims for inpatient and outpatient services by institutional facilities (for example, outpatient departments, rural health clinics, chronic. Web learn how to fill out the ub04 form for health insurance claims with this online tutorial from mcgraw hill education. Web patient control number enter your. Billing provider name & address. We are providing two different versions in. Enter the billing provider’s mailing. Enter the name and address of the hospital/facility submitting the claim. This number will be printed on the ra and will help. • inpatient hospital facilities, such as medical/surgical intensive. Web the ub04 claim form is used to submit claims for inpatient and outpatient services by institutional facilities (for example, outpatient departments, rural health clinics, chronic. Billing provider name & address. Web patient control number enter your facility's unique account number assigned to the patient, up to 20 alpha/numeric characters. Enter the. Enter the billing provider’s mailing. Web of essential information as requested by this form, may serve as the basis for civil monetarty penalties and assessments and may upon conviction include fines and/or. You can fill in the attached forms electronically, using adobe form filler, as long as you have adobe acrobat reader. This number will be printed on the ra. Online customers supportpaperless workflowfree trialcancel anytime Web of essential information as requested by this form, may serve as the basis for civil monetarty penalties and assessments and may upon conviction include fines and/or. • inpatient hospital facilities, such as medical/surgical intensive. Web the ub04 claim form is used to submit claims for inpatient and outpatient services by institutional facilities (for. Billing provider name & address. You can fill in the attached forms electronically, using adobe form filler, as long as you have adobe acrobat reader. Enter the billing provider’s name, street address, city, state, and zip code where the services were performed. Web the ub04 claim form is used to submit claims for inpatient and outpatient services by institutional facilities (for example, outpatient departments, rural health clinics, chronic. Enter the name and address of the hospital/facility submitting the claim. This number will be printed on the ra and will help. Online customers supportpaperless workflowfree trialcancel anytime Web of essential information as requested by this form, may serve as the basis for civil monetarty penalties and assessments and may upon conviction include fines and/or. Enter the billing provider’s mailing. • inpatient hospital facilities, such as medical/surgical intensive.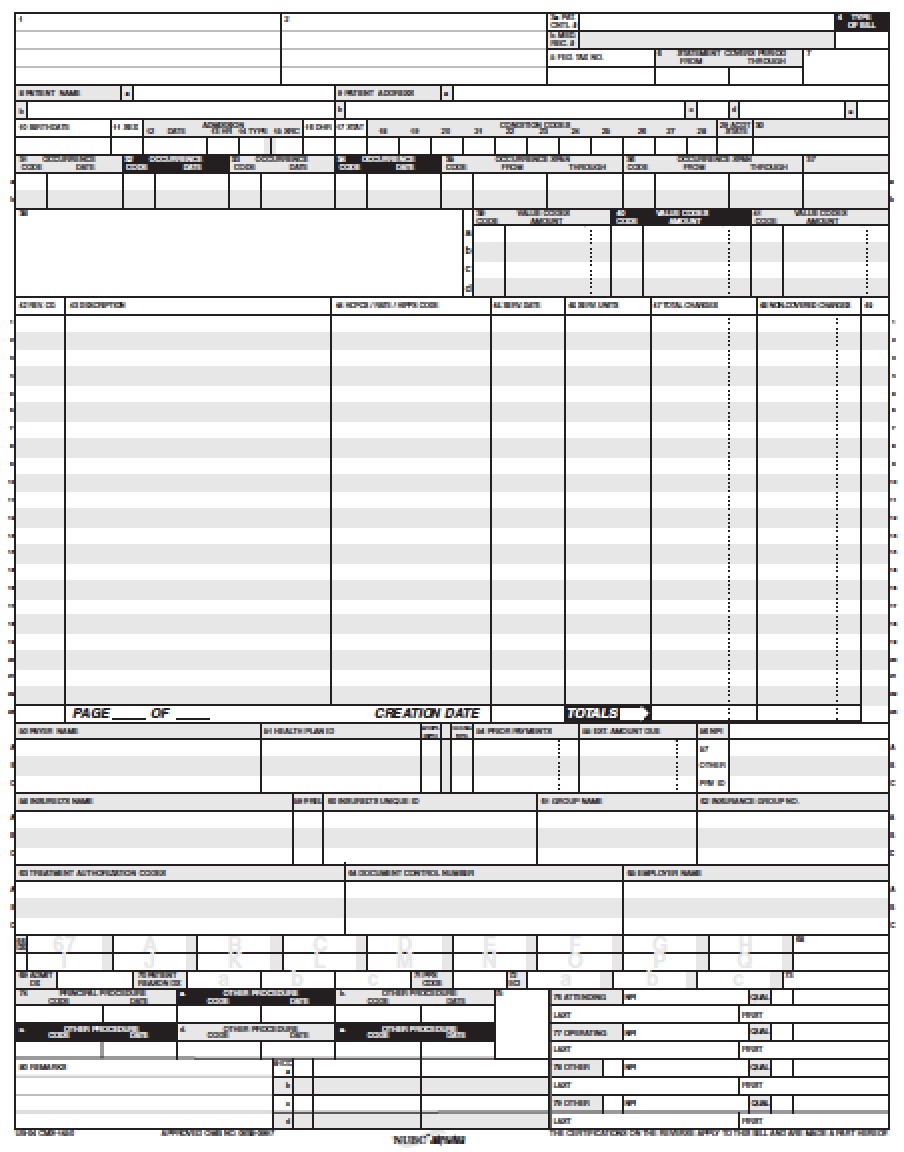
Download UB04 Claim Form PDF wikiDownload
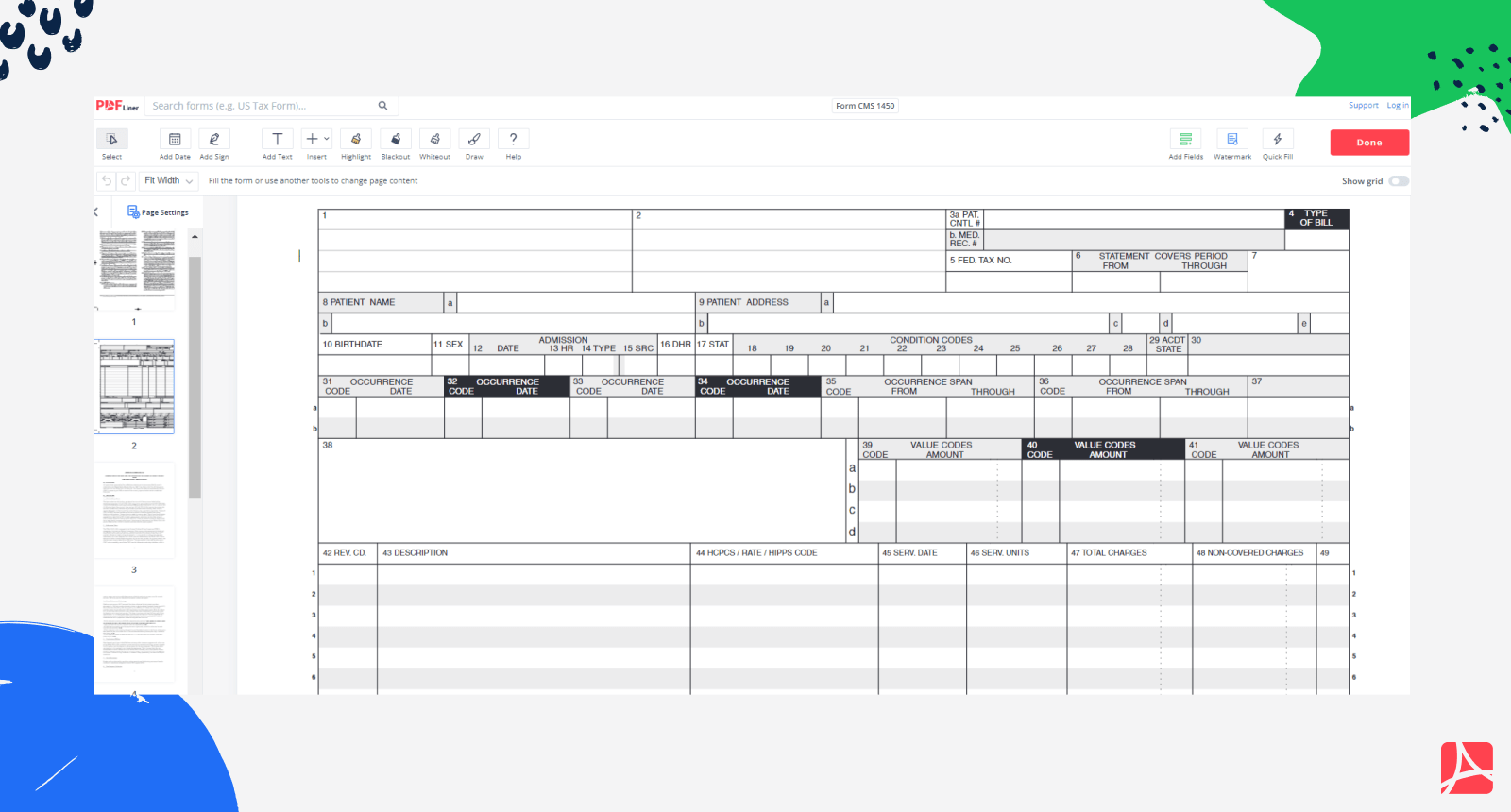
UB04 Form or CMS 1450 Print and sign form CMS 1450 online — PDFliner
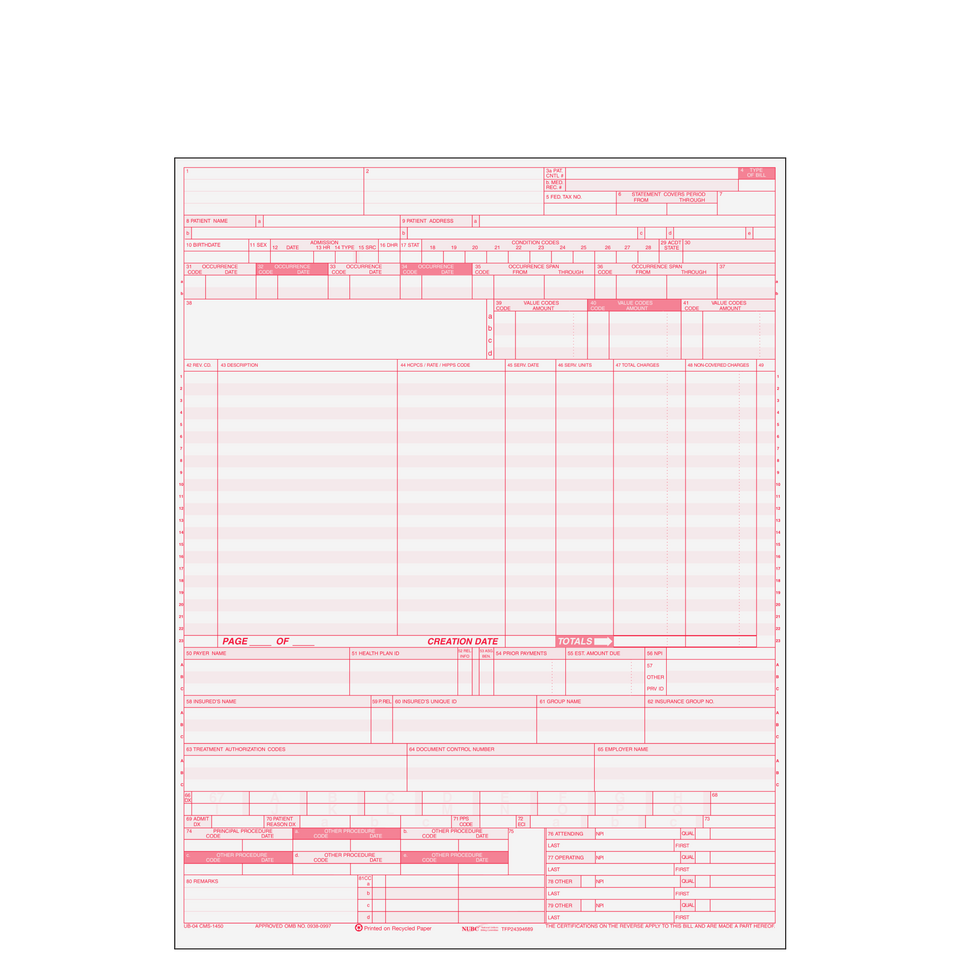
UB04CF UB04 Hospital Claim Form
Ub04 Ms Word Form Fill and Sign Printable Template Online US Legal
NUBC UB04 CMS1450 Fill and Sign Printable Template Online US Legal
Free Fillable Ub 04 Claim Form Printable Forms Free Online
Blank Ub 04 Claim Form Printable
Ub 04 Fillable Template Master of Documents
Ub 04 Form Tricare Bill Form printable pdf download
Free Fillable And Printable Ub 04 Claim Form Printabl vrogue.co
Web Learn How To Fill Out The Ub04 Form For Health Insurance Claims With This Online Tutorial From Mcgraw Hill Education.
Web Patient Control Number Enter Your Facility's Unique Account Number Assigned To The Patient, Up To 20 Alpha/Numeric Characters.
We Are Providing Two Different Versions In.
Related Post: